Understand the Flow Before Intervening — Why CHIVA Places Methodological Weight Preoperatively
Core Summary
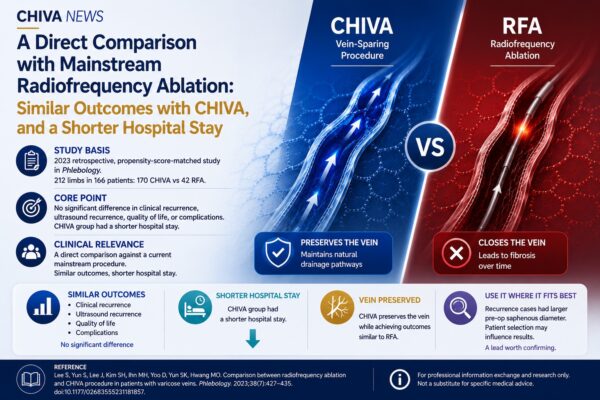
Study Basis: In 2015, Gianesini and seven coauthors from the Vascular Disease Center at the University of Ferrara published CHIVA strategy in chronic venous disease treatment: instructions for users in Phlebology, systematically outlining the full operational pathway of CHIVA, from ultrasound assessment and hemodynamic classification to surgical decision-making.
Key Judgment: The article translates CHIVA from a conceptual “approach” into a step-by-step guide for practitioners, repeatedly emphasizing a central fact — the effectiveness of CHIVA depends on whether it is correctly understood and correctly executed.
Clinical Implication: This methodological clarification provides an early blueprint for integrating CHIVA into systematic physician education and training frameworks, highlighting that for broader clinical adoption, accurate learning of the method is essential.
⸻
In clinical practice, a repeatedly observed phenomenon is that two doctors who claim to perform CHIVA may deliver different treatments. This variation is not always due to experience level; more often, it reflects incomplete understanding of the method itself — key points in ultrasound assessment may be simplified, shunt classifications skipped, and procedural choices made based on habit rather than flow distribution. CHIVA’s effectiveness relies on methodological adherence; deviations quickly reduce reproducibility. Gianesini et al.’s 2015 review addresses this issue. It does not re-discuss CHIVA’s efficacy but instead asks: what must a physician understand, and in what sequence should steps be executed to perform CHIVA accurately?
1. CHIVA as an Executable Workflow
The phrase “instructions for users” in the title is critical. The authors target physicians willing to attempt CHIVA but lacking a complete methodological pathway, noting that part of CHIVA’s slow adoption stemmed from perceptions of it being “indirect” or “not straightforward.”
The article divides CHIVA into four interconnected stages — preoperative ultrasound assessment, hemodynamic classification, procedural decision-making, and postoperative follow-up — each written as identifiable, teachable, and externally verifiable decision points. This structure implies that unless CHIVA can be reduced to learnable steps, it remains a personal skill rather than a standardized method.
2. The Hardest Part Happens “Before the Hands-on Work”
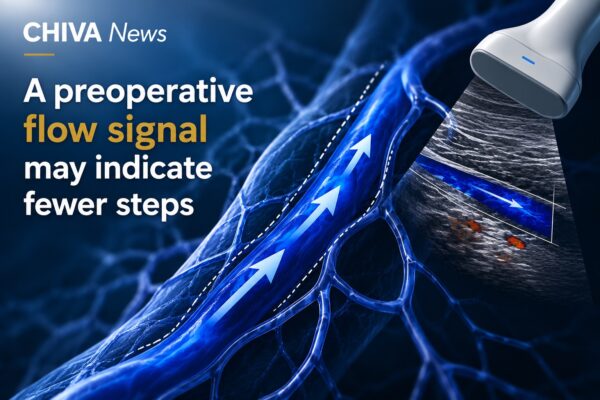
The article emphasizes preoperative assessment. Identifying reflux origins, mapping flow in the standing position, distinguishing shunt types, and evaluating perforator function — these elements, often background in conventional surgical reviews, are central here.
This addresses a common misconception: CHIVA is not simply a collection of ligation sites but a judgment system based on individual flow patterns. Learning “what to do” without understanding “why” leads to variable clinical delivery under the same procedural labels.
3. Procedural Classification as a Decision Tree
CHIVA procedure types (CHIVA 1, CHIVA 2, CHIVA 1+2, etc.) are presented in previous literature as lists. Gianesini et al. instead strictly map each procedure to shunt type, forming a decision tree.
For new CHIVA practitioners, the decision tree removes uncertainty: the choice is no longer “which CHIVA should I select?” but “which procedure corresponds to the identified shunt?” This transformation from experience-based to process-based decision-making is key to scalable and replicable practice.
4. Clinical Perspective: Methodology First Enables Training and Standardization
From today’s perspective, the significance of this review is not only producing an operational guide but demonstrating how CHIVA can be systematized.
A strategy can only enter broad physician education if it can be clearly taught, decomposed into assessable competencies, and organized into verifiable steps. Without these prerequisites, subsequent training, certification, and cross-center quality control cannot be implemented.
This is why the review remains widely cited: it does not provide new evidence of CHIVA’s effectiveness but shows how a “non-originator” physician can accurately learn and execute it. CHIVA is moved from reliance on a few highly skilled operators to a method that can be systematically taught. Viewed alongside today’s Global CHIVA Program and structured training frameworks, this review prefigures such methodological work. It highlights that global CHIVA adoption depends not only on acceptance but on accurate teaching and execution — the true work of physician education and standardization.
Reference
Gianesini S, Occhionorelli S, Menegatti E, Zuolo M, Tessari M, Spath P, Ascanelli S, Zamboni P. CHIVA strategy in chronic venous disease treatment: instructions for users. Phlebology. 2015 Apr;30(3):157–171. doi: 10.1177/0268355514531953.
About the Authors
The study was led by Sergio Gianesini and his team at the University of Ferrara Vascular Disease Center. Last author Paolo Zamboni is the head of the center and a representative scholar within the CHIVA system. The Ferrara School in Italy remains one of the most active academic centers for CHIVA, continuously producing standardized literature on ultrasound assessment, hemodynamic classification, and methodological teaching.
Note: This article is based on publicly available literature for professional information exchange and research purposes; it does not constitute specific medical advice.