What Happens to Ulcer Outcomes in PTS Patients When the Great Saphenous Vein Is Missing?
Key Points
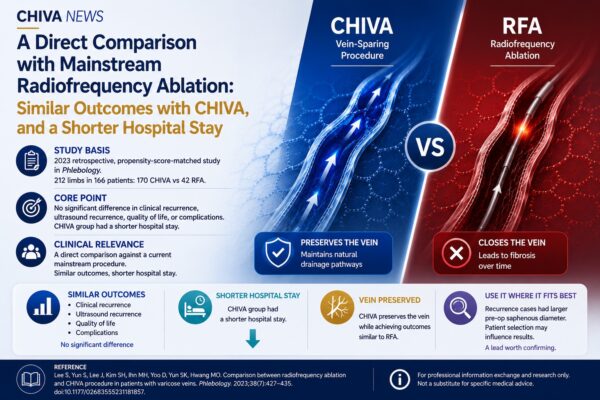
•Study basis: A 2024 retrospective comparative study published in the Journal of Vascular Surgery: Venous and Lymphatic Disorders examined the relationship between the presence or absence of the great saphenous vein and ulcer healing and recurrence in patients with post-thrombotic syndrome (PTS) and active venous ulcers.
•Core finding: In this patient group, those with a preserved great saphenous vein showed higher healing rates, faster healing, and lower long-term recurrence.
•Clinical implication: The study suggests that in complex venous disease, the significance of the great saphenous vein should not be judged only from the perspective of reflux; its functional role within the venous return system may deserve renewed attention.
In many treatment pathways for varicose veins, the great saphenous vein is often viewed as the most direct target for intervention.
But in more complex venous disease, that way of thinking may not always be sufficient.
This 2024 retrospective study, published in the Journal of Vascular Surgery: Venous and Lymphatic Disorders, focused on patients with post-thrombotic syndrome complicated by active venous ulcers. In this group, the deep venous system is often already compromised, and venous return pathways and pressure distribution are usually far more complex than in uncomplicated varicose vein disease.
The central question of the study was not the superiority of one specific procedure.
Instead, it addressed a more basic clinical issue:
what happens to healing and long-term outcomes when the great saphenous vein is no longer present.
1. Study Design and Patient Characteristics
The study focused on patients with PTS in the C6 stage, meaning patients with active venous ulceration.
At this stage, impairment of the deep venous system is often substantial, and venous return may depend on multiple pathways working together.
Under these conditions, the role of the great saphenous vein may no longer be limited to that of a “refluxing superficial vein.”
In some patients, it may also contribute to venous return compensation and pressure buffering.
Against this background, the investigators divided patients into two groups:
those in whom the great saphenous vein was still present, and those in whom it was absent, then compared ulcer healing and long-term recurrence between the two groups.
The design of the study was straightforward, but the clinical question was important:
in a complex venous hemodynamic setting, is the great saphenous vein truly a vein that can be given up without consequence?
2. Main Results
The results showed clear differences between the two groups across several key outcomes.
First, ulcer healing rate.
Patients with a preserved great saphenous vein had a healing rate of 97%, whereas the healing rate in the absent-vein group was 71%.
Second, healing time.
The median healing time in the absent-vein group was 161 days, compared with 42.5 days in the preserved-vein group.
Third, long-term recurrence rate.
The recurrence rate in the absent-vein group reached 85%, suggesting a much less favorable long-term course.
Taken together, these findings point in one consistent direction:
in this patient population, the presence of the great saphenous vein was associated with better healing and more stable long-term outcomes.
3. From “Whether to Treat It” to “How to Understand Its Function”
The significance of these findings goes beyond the data themselves.
In traditional treatment logic, a refluxing vein is often seen mainly as a structure that needs to be treated.
But this study suggests that in a more complex hemodynamic environment, the meaning of the great saphenous vein is not always so simple.
For some patients, it may participate not only in abnormal reflux, but also in venous return redistribution and pressure regulation.
When that functional role is overlooked, treatment may do more than eliminate a source of reflux; it may also weaken an existing compensatory pathway.
This shifts the question of whether the great saphenous vein should be preserved from a purely technical choice to a broader issue of how the venous return system is understood.
Whether a vein should be treated cannot be determined by reflux alone. It must also be interpreted in the context of pressure relationships and functional distribution within the entire venous system.
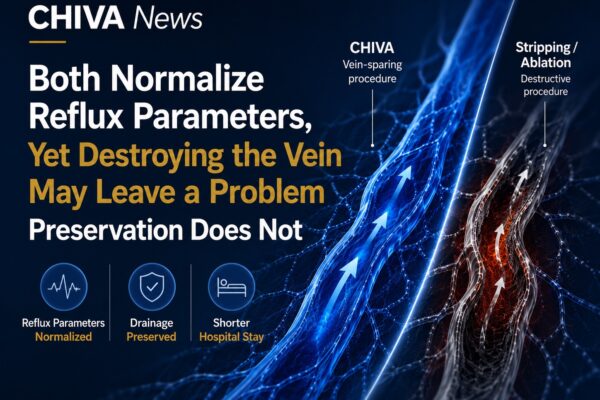
This also helps explain why the CHIVA treatment approach, characterized by preservation of the great saphenous vein and hemodynamic correction, has been receiving renewed attention in recent years.
From this perspective, what the study raises is not only a difference in outcomes within one patient group, but a more fundamental clinical question:
in the long-term management of venous disease, should greater emphasis be placed on preserving function, compensatory capacity, and hemodynamic balance?
⸻
Reference:
Bishara RA, et al. Impact of great saphenous vein ablation on healing and recurrence of venous leg ulcers in patients with post-thrombotic syndrome: A retrospective comparative study. J Vasc Surg Venous Lymphat Disord. 2024 Mar;12(3):101859.
Note:
This article is based on publicly available literature and is intended for professional communication and content reference only. It does not constitute specific medical advice.