From “Removal” to “Correction”: A 2023 Review Re-emphasizes the True Positioning of CHIVA
Key Points
• Article background:
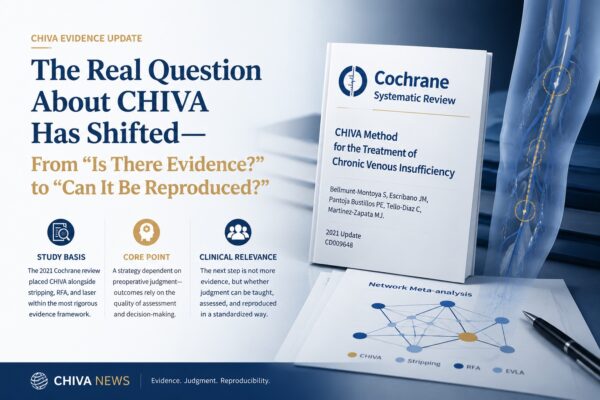
In 2023, Roberto Delfrate published a review in the Journal of Theoretical and Applied Vascular Research discussing the positioning of CHIVA in the treatment of venous insufficiency.
• Core judgment:
The article argues that CHIVA is not simply a set of surgical maneuvers, but a treatment strategy built on hemodynamic reasoning.
• Clinical focus:
The paper repeatedly emphasizes that standardized ultrasound assessment, treatment mapping, and the learning curve are key factors determining whether CHIVA can truly be implemented well in practice.
In the treatment of varicose veins and venous insufficiency, the physician is never dealing with just one simple question: whether or not a particular vein segment should be treated. The real issues are where the abnormal pressure comes from, how reflux is formed, which flows should be preserved, and which connection points actually need to be interrupted.
This is precisely the focus of Roberto Delfrate’s 2023 article. It is not trying to prove whether CHIVA “works,” nor is it simply repeating the value of preserving the great saphenous vein. Instead, it places CHIVA back where it originally belongs: first as a treatment strategy, and only then as an intervention.
Background and Design of the Review
This paper is a review article. At the very beginning, the author divides the treatment of venous insufficiency into two broad paths. One leans toward “removing problematic veins,” while the other leans toward “first understanding how pressure overload and reflux are formed, and then deciding how to intervene.”
CHIVA clearly belongs to the latter.
For that reason, the article does not begin with operative steps, but with the logic of clinical judgment. The author stresses that truly understanding CHIVA does not start with memorizing procedure names. It starts with accurate and standardized color Doppler ultrasound assessment, followed by treatment mapping based on hemodynamic relationships. In other words, if the upstream judgment is wrong, the downstream procedure can no longer truly be called CHIVA.
What the Article Is Really Emphasizing
There is an important reminder in this article.
It points out that not every blood flow pattern that “looks abnormal” in the venous system should be eliminated automatically. The author notes that whether blood flow is antegrade or retrograde, if it is serving a useful drainage function within the local circulation, it may still deserve to be preserved.
This is also one of the most fundamental differences between CHIVA and many approaches that treat reflux simply because reflux is seen.
So what this article is really trying to say is not that CHIVA is somehow “special” in itself, but that physicians need to learn how to read venous hemodynamics correctly. If that is not done well, “vein preservation” may become only a superficial preservation. If it is done well, then the goal of treatment is no longer just to “remove the diseased segment,” but to reorganize pressure and drainage.
The Threshold of CHIVA Is Precisely What Gives It Methodological Value
This article also carries an important practical message: it does not describe CHIVA as a technique that “anyone can easily perform.”
On the contrary, the author explicitly states that CHIVA has a learning curve. Without correct hemodynamic assessment and mapping, what follows may become what is referred to as “bad CHIVA.”
This point matters.
Because it shows that the challenge of CHIVA does not lie only in surgical actions, but in the understanding and judgment that come before them. Learning a local maneuver does not mean that one has truly mastered CHIVA. The real threshold lies in whether one can stably and consistently perform assessment, analysis, and strategy planning in a standardized way.
Seen from this angle, the threshold of CHIVA is not its weakness. It is precisely what distinguishes it from more generic “treatment-oriented” procedures. CHIVA does not require only technical dexterity. It requires training in an entire methodology.
Moving the Discussion Back from Technique to Treatment Logic
One of the most valuable contributions of this article is that it pulls CHIVA away from the superficial impression of being merely a “vein-preserving” treatment.
When many people hear CHIVA, their first reaction is that it avoids burning, avoids stripping, and tries to preserve the great saphenous vein. All of that is true. But if the discussion stops there, CHIVA is easily understood too narrowly.
What Delfrate wants to emphasize is that the value of CHIVA does not lie only in what it preserves, but in the fact that it builds treatment on pathophysiology and hemodynamic reasoning. It requires the physician to understand why venous hypertension appears, why abnormal reflux develops, and then decide where interruption is needed and where preservation is appropriate.
In other words, the core of CHIVA is not simply that it is “more conservative,” but that it is “more strategic.”
That is why this review still matters today. It does not remain at the level of procedure labels. Instead, it brings the discussion back to one of the most fundamental questions in venous disease treatment:
Are we treating a vein segment, or are we treating a pressure system?
Reference:
Delfrate R. CHIVA strategy in the treatment of venous insufficiency. Journal of Theoretical and Applied Vascular Research. 2023;8(2):17–32. Published Aug 31, 2023.