Both Normalize Reflux Parameters, Yet Destroying the Vein May Leave a Problem Preservation Does Not
Key Takeaways
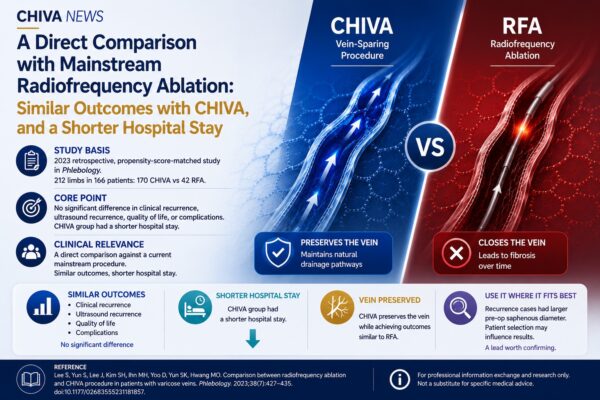
• Study basis: In 2023, Cappelli, Molino Lova, Pinelli, and Franceschi published a short review in the Journal of Theoretical and Applied Vascular Research comparing the differing hemodynamic effects of destructive procedures (stripping, endovenous ablation) and vein-sparing procedures (CHIVA) after reflux is corrected.
• Core point: Both types of procedure can significantly improve plethysmographic reflux parameters to normalization; however, the available data suggest that destructive procedures may reduce lower-limb compliance and affect drainage of the superficial tissue, whereas an appropriately performed vein-sparing procedure can preserve this drainage function.
• Clinical relevance: Bringing reflux-related parameters back to normal is only half of the outcome; what drainage capacity the venous system retains after treatment is where a vein-sparing strategy deserves attention.
The most direct measure of a venous treatment is whether reflux is corrected. Judged by plethysmographic reflux parameters, stripping, ablation, and CHIVA all achieve this — all can bring these parameters back to normal. But this review asks a further question: once the reflux parameters are normalized, is the hemodynamics of the limb really the same?
1. After reflux parameters normalize, the two types are not the same
The review first analyzes the hemodynamic changes brought by destructive and by vein-sparing procedures, then compares their effects on the long-term course of varicose disease, and on recurrence in particular.
On improving reflux parameters, both types reach normalization — plethysmography shows that destructive and vein-sparing procedures alike bring reflux parameters back to normal. The difference lies elsewhere: the available data suggest that destructive procedures may reduce lower-limb compliance, and in turn affect drainage of the superficial tissue.
The authors describe a specific observation: after the vein is destroyed, a form of recurrent varicose veins can appear in which no clear trans-fascial reflux point is found. The authors argue that this kind of recurrence cannot be explained by a conventional trans-fascial reflux point alone, and is more likely related to impaired drainage of the superficial tissue; in the vein-sparing literature they review, such recurrence is not reported. On this basis, the authors propose that a vein-sparing procedure, performed appropriately according to the shunt type, can preserve superficial-tissue drainage and make an otherwise incompetent venous system more hemodynamically stable.
It should be said plainly that this is a short review from one strand of hemodynamic research; its conclusions are synthesized from different studies rather than drawn from a single trial directly comparing all the relevant measures across both procedure types, and should be read accordingly.
2. This difference points to a layer beyond reflux
Put together, the two points shift the focus of the comparison.
The question is no longer only “which can correct reflux” — both improve reflux-related parameters; it is also what drainage capacity the venous system retains after treatment. Correcting reflux and maintaining drainage are not the same question. A destructive procedure, while improving reflux parameters, also removes the saphenous vein’s role as a drainage channel; an appropriately performed vein-sparing procedure corrects reflux while preserving that channel.
The recurrence with no detectable reflux point is a notable signal here: it suggests that destroying the vein may create a hemodynamic problem that cannot be explained by a detectable reflux point alone, and one that, in the authors’ data, is not seen after vein-sparing treatment. Under the shared result of “reflux parameters improved,” preservation may retain a drainage advantage that destruction is less able to offer. This hemodynamic account also offers one possible way of understanding the finding, in the 2019 network meta-analysis by Guo et al., that CHIVA ranked among the highest for long-term recurrence outcomes.
3. Clinical perspective: the endpoint of treatment is not reflux alone
Seen this way: judging a venous procedure should look not only at whether it improved reflux parameters, but at what state the limb’s drainage is left in afterward. And an appropriately performed vein-sparing strategy is precisely aimed at preserving that layer.
If outcome assessment comes to include dimensions beyond reflux correction — compliance, drainage, and the morphology of recurrence — the hemodynamic case for preserving the vein will also become clearer. Correcting reflux is only one step; what influences the long-term state of the limb is not only whether reflux is corrected, but also what drainage capacity is retained after treatment.
⸻
References: Cappelli M, Molino Lova R, Pinelli M, Franceschi C. Are saphenous sparing treatments beneficial to the hemodynamics of the venous system? Journal of Theoretical and Applied Vascular Research. 2023;8(1):33–37. doi:10.24019/jtavr.149.
About the authors: This review was conducted by Massimo Cappelli and Raffaele Molino Lova (Private Practice, Florence, Italy), Mauro Pinelli (Private Practice, Avezzano, Italy), and Claude Franceschi (Hôpital Saint Joseph, Paris, France), and published in the Journal of Theoretical and Applied Vascular Research.
Disclaimer: This article is compiled from publicly available literature for the purpose of professional information exchange and content research. It does not constitute specific diagnostic or treatment advice.
About CHIVA News: This column is produced by GCM (Global CHIVA Management). We are dedicated to tracking and sharing the latest academic developments, literature analyses, and clinical-practice discussions in the field of hemodynamic treatment of lower-limb venous disease worldwide, providing rigorous and objective medical information for clinical professionals.