What Makes CHIVA Difficult Is Not the Procedure Alone
Key Points
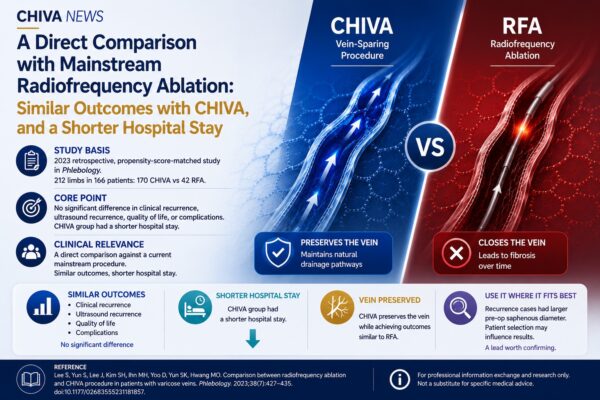
- Study basis: In 2024, Stefano Ricci published CHIVA for dummies in Phlebology, focusing on the practical barriers to the wider clinical adoption of CHIVA.
- Core judgment: The article argues that one major reason CHIVA has not spread more broadly is the common belief that it requires highly advanced duplex ultrasound expertise.
- Clinical focus: The author suggests that preserving the great saphenous vein does not necessarily require extremely complex hemodynamic analysis in every case, and that entry into this treatment approach may be built around a limited number of key judgments.
When CHIVA is discussed, the first things many people think of are “great saphenous vein preservation,” “hemodynamic correction,” and “preoperative mapping.”
But if the question is pushed one step further, what really limits its dissemination is often not the concept itself, but something more practical: how an ordinary venous disease specialist can actually enter and learn this method.
That is the main focus of Stefano Ricci’s 2024 article, CHIVA for dummies.
The paper is not trying to downplay the methodological demands of CHIVA. Rather, it addresses a long-standing clinical barrier more directly: if CHIVA is always understood as a highly complex system that can only be mastered by a small number of specialists, it will remain difficult for the method to enter broader routine practice.
1. The Article Is About How CHIVA Enters Clinical Practice
From the published abstract, Ricci first revisits the basic background of CHIVA. The method was introduced by Claude Franceschi in 1988 as a treatment strategy centered on preserving the great saphenous vein. At the same time, the article points out that CHIVA has long struggled to spread more widely because it is commonly perceived as requiring advanced duplex ultrasound expertise and highly individualized planning for each patient.
For that reason, the real question of the paper is not simply what CHIVA is, but something more practical:
if CHIVA is to be truly mastered by more physicians, where is the entry point for learning it?
This is what makes the article different from a standard methodological review. Instead of pushing the discussion toward more complexity, it tries to clarify which judgments are truly essential for great saphenous vein–preserving treatment, and which parts can be reduced to a more basic and learnable clinical pathway.
2. What the Article Tries to Reduce Is the Entry Barrier, Not the Methodological Value
From the abstract, the author makes one point especially clear:
achieving great saphenous vein–preserving treatment does not always require extremely complex analysis of every hemodynamic detail. Instead, the learning process may be organized around a limited number of key clinical assessments.
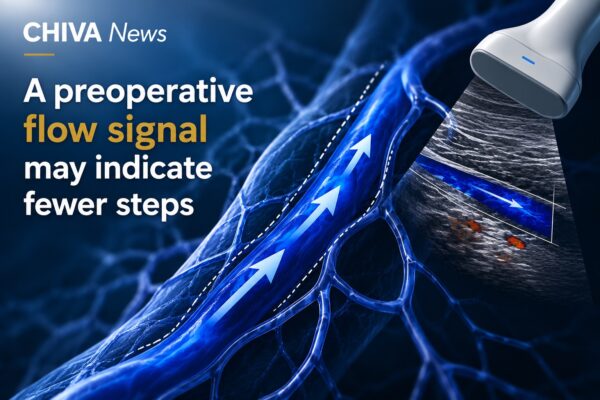
The PubMed summary notes that basic ultrasound skills may already support entry into this treatment logic, particularly through recognition of two essential elements:
the functional status of the saphenofemoral junction and the location of refluxing perforators.
What matters most here is not the suggestion that “CHIVA is simple.”
What matters is that the paper makes the learning problem more concrete. If a method remains defined only by complexity and difficulty of access, it is unlikely to move beyond conceptual approval into wider clinical use.
The conclusion also notes that, in order to achieve the goal of conservative great saphenous vein treatment, limited phlebectomy combined, when needed, with saphenofemoral junction interruption may represent a more simplified solution. The important point is not any individual maneuver, but the author’s attempt to move CHIVA from being merely “theoretically correct” toward being “clinically learnable.”
3. The Real Difficulty Still Lies in Judgment, Not in Copying a Technical Move
The value of this article is not that it lowers the standards of CHIVA, but that it reminds readers where the real challenge has always been.
What makes CHIVA difficult is not simply how to perform it, but what must be judged before anything is done.
If those judgments cannot be taught, transferred, and structured, then even a strong therapeutic concept will remain difficult to implement consistently. On the other hand, if the learning pathway can be built around a few decisive judgments, CHIVA no longer has to remain a method practiced only by a small number of experts.
Seen from this angle, Ricci is not raising a purely theoretical issue.
He is asking a very practical clinical question:
if a treatment strategy is to enter real-world practice, it is not enough to show that it works — it must also become teachable.
That is what gives this article a distinct place within the CHIVA News series. Earlier articles focused more on outcomes, long-term value, or the significance of preserving the vein itself. This one shifts the discussion to another level: how CHIVA moves from being understood to being truly learned.
⸻
Reference:
Ricci S. CHIVA for dummies. Phlebology. 2024 May;39(4):238–244. doi:10.1177/02683555231225788.
Note:
This article is based on publicly available literature and is intended for professional communication and content reference only. It does not constitute specific medical advice.